



Bridging generational gaps in ethnomedicinal knowledge
From the perspective of age distribution and its implications for identifying medicinal plants, we collected data across seven age groups: 30–39, 40–49, 50–59, 60–69, 70–79, 80–89, and 90 or older (Table 2). We formulated the null hypothesis (H0) that there is no significant difference in medicinal plants knowledge across these age groups. Conversely, the alternative hypothesis (H1) proposes that there are notable differences. Since the data exhibited unequal variances and were not normally distributed, we employed the Kruskal–Wallis H-test to compare the groups.
The calculated Kruskal–Wallis H statistic was 17.751, with a p-value of 0 0.007 (p < 0.05). Therefore, the null hypothesis (H0) was rejected at the 5% significance level, confirming that knowledge about the number of medicinal plants varies significantly across the evaluated age groups. Findings indicate that individuals aged 40–49 possess the most extensive knowledge of medicinal plants, followed by those in the 50–59, 70–79, 60–69, and 80–89 age brackets. It is plausible that middle-aged populations (40–59 years) have accumulated substantial knowledge through experiential learning and active engagement with traditional medicinal systems. Conversely, younger adults (30–39 years) and elders (aged 90 and above) demonstrate the lowest levels of knowledge, potentially due to a shift towards modern pharmaceutical practices amongst younger cohorts and age-related cognitive decline among older adults. This may be due to impaired memory and reduced participation in traditional medicinal practices. This trend underscores the influence of lifestyle changes and cognitive factors on the retention and transmission of ethnomedicinal knowledge. Additionally, the study aimed to explore the frequency of medicinal plants used across different age groups using Fisher’s exact test. The null hypothesis (H0) states that there is no significant difference in medicinal plant use among the age groups, while the alternative hypothesis (H1) proposes that such differences do exist. The results yielded a p-value of 00.019 (p < 0.05), leading to the rejection of the null hypothesis at the 5% significance level. This indicates a statistically significant difference in the frequency of medicinal plant use across age groups. The middle-aged groups and elders, specifically those aged 50–59, 60–69, and 70–79 years, demonstrated a significantly higher frequency of using medicinal plants. In contrast, younger adults aged 30–39 and very elderly individuals aged 90 and above reported lower utilization of medicinal plants. These findings underscore the impact of age on traditional medicinal practices and suggest a potential generational shift in the reliance on or knowledge of medicinal plant use. Furthermore, the study also assessed the depth of traditional knowledge about medicinal plants among different age groups, measured by the number of recognized medicinal plants, their various uses, and understanding of culturally essential practices. The null hypothesis (H0) states that traditional knowledge does not significantly vary among age groups, whereas the alternative hypothesis (H1) suggests there are significant differences. A Chi-square test of independence was conducted, producing a Chi-square statistic of 31. 253 and a p-value of 0 0.001 (p < 0 0.05). This strong evidence led to rejecting the null hypothesis at the 5% significance level, confirming that there are statistically significant differences in traditional knowledge among age groups. The present research indicates a trend in the understanding of conventional medicine across different age groups within the Tripuri people. Specifically, individuals aged 50–59, 60–69, and 70–79 demonstrate a solid grasp of traditional medicinal practices. In contrast, those aged 30–39 and 40–49 generally possess a more basic comprehension of ethnomedicine. This suggests that elderly individuals have a richer understanding of the application and cultural significance of medicinal plants compared to their younger counterparts. The findings highlight the importance of age-related experience and knowledge retention in the context of traditional healing practices.
Understanding and application of medicinal plants according to gender
To achieve the goal, we consider the null hypothesis (H0) that there are no differences in the understanding of medicinal plants across genders. In contrast, the alternative hypothesis (H1) is that significant differences exist. Given that the group variances are not homogeneous, and the samples diverge from a normal distribution, the Mann–Whitney U test was employed to evaluate the potential influence of gender on knowledge of the number of medicinal plants. The computed Mann–Whitney U statistic was 2440, while the p-value for this test was 0.000 (p < 0.05). Consequently, H0 was rejected at the 5% significance level. The study reveals a significant variation in knowledge of medicinal plants between male and female participants. Specifically, male participants demonstrate a more comprehensive understanding of medicinal plants compared to females. This suggests gender differences in interactions with, learning about, and utilization of medicinal plants, which may have implications for both traditional knowledge systems and future research on plant-based medicine. Further investigation could explore the factors contributing to these disparities, such as cultural practices, education, and environmental interactions (Table 2). A Chi-square test was conducted to assess the frequency of medicinal plant usage across genders. The calculated Chi-square statistic was 17.124, with a corresponding p-value of 0.000 (p < 0.05). Thus, the null hypothesis (H0) was rejected at the 5% significance level, indicating that male participants demonstrate a significantly higher frequency of medicinal plant utilization compared to female participants. Furthermore, a separate Chi-square test was performed to evaluate the influence of gender on traditional knowledge of medicinal plants. The resulting Chi-square statistic for this analysis was 33.974, with a p-value of 0.000 (p < 0.05). This also resulted in the rejection of the null hypothesis (H0) at the 5% significance level, suggesting that there is a significant difference in traditional knowledge of medicinal plants between genders. Specifically, male participants demonstrated a greater understanding of traditional medicine compared to female participants, as males are more likely to be engaged with ethnomedicinal practices.
The connection between participants’ education and their understanding of the uses of medicinal plants
Most informants reported completing their primary education, while 18% remained illiterate. However, it is worth noting that individuals with formal and informal education (formally illiterate) demonstrated a profound understanding of the usage of various medicinal plants. The Kruskal–Wallis H-test was employed to assess the relationship between educational attainment, awareness of traditional medicinal flora, and the frequency of utilization for different health conditions. To reach our goal, we define a null hypothesis (H0) stating there is no meaningful difference between educational qualification and knowledge or use of medicinal plants. Conversely, the alternative hypothesis (H1) suggests that significant differences do exist. The Kruskal–Wallis H statistic yielded a value of 3.751 and a p-value of 0.290 (p > 0.05). Consequently, H0 could not be rejected at a 5% significance level, indicating that understanding the number of medicinal plants does not statistically differ among diverse educational backgrounds. Individuals without formal education reported an average of 14 plant species, while those with primary education reported an average of 18 species. In contrast, individuals with secondary education identified approximately 15 species, and those holding graduate degrees reported an average of 17 plant species. The understanding of medicinal plants and their utilization by the Tripuri people represents a rich intersection of ethnomedicinal knowledge and cultural heritage. Since the utilization of medicinal plants is primarily transmitted through oral presentations by traditional healers and elders, it highlights the importance of intergenerational learning in preserving traditional wisdom. The medicinal plants are not only a source of therapeutics but also have deep cultural value. Therefore, from childhood, this knowledge is transmitted, and a lack of formal education does not hinder the acquisition of knowledge; instead, it underscores the effectiveness of experiential learning within their cultural framework. This tradition emphasizes a profound relationship with nature, where understanding and respect for medicinal plants are integral to the community’s identity and health practices. In examining the frequency of medicinal plant usage across different academic backgrounds, we formulate the null hypothesis (H0) as stating that there are no significant differences between educational background and the usage of medicinal plants. The alternative hypothesis (H1) posits that differences do exist. The Chi-square statistic recorded for the frequency of medicinal plant usage across varying educational levels was 2.275, with a p-value of 0.321 (p > 0.05). Hence, H0 could not be rejected at a 5% significance level, indicating that the frequency of medicinal plant utilization does not significantly differ by educational attainment, as the Tripuri people understand the use of medicinal plants from childhood and gain experience with age. Additionally, we examined whether educational level influences self-reported effectiveness of medicinal plants. We formulated the null hypothesis (H0): the self-reported effectiveness of medicinal plants is not significantly different across various educational levels. Conversely, the alternative hypothesis (H1) states that the self-reported effectiveness of medicinal plants differs significantly across different educational levels. The p-value from Fisher’s exact test was 0.142, which exceeds the threshold of 0.05. Therefore, the self-reported efficacy of medicinal plants does not vary significantly across different educational levels, as this tribe maintains strong cultural beliefs in traditional healing practices and chooses medicinal plants based on experiential knowledge rather than scientific validation.
Influence of profession on knowledge of medicinal plants and their utilization
The majority of the informants surveyed were farmers, accounting for 51% of the respondents. This was followed by traditional healers at 17%, housewives at 15%, government employees at 9%, and traders at 8%. To assess the impact of the participants’ professions on their knowledge of medicinal plants, we formulated a null hypothesis (H0) which states that there is no significant difference in understanding of medicinal plants across different occupations. In contrast, the alternative hypothesis (H1) posits that there is a significant difference in this knowledge among various occupations. The analysis yielded a Kruskal–Wallis H statistic of 25.085 with a p-value of 0.000 (p < 0.05). As a result, we rejected the null hypothesis at the 5% significance level, concluding that knowledge of medicinal plants varies significantly among different occupations. The data revealed that traditional healers had an average understanding of 48 medicinal plants, while traders averaged 13, government employees approximately 11, and both farmers and homemakers averaged around 10 plants. Traditional healers, who formed the primary group of informants, typically gain their expertise over the years through practice in ethnomedicine. It was also found that traditional healers, traders, and government employees frequently used medicinal plants. Specifically, 75.2% of farmers and 70.8% of housewives reported using these plants regularly, while 18.4% of farmers and 8.3% of housewives occasionally used them. Only 6.4% of farmers and 20.8% of housewives stated that they rarely used medicinal plants.
Furthermore, traders, housewives, and government employees exhibited advanced knowledge of these plants. Basic traditional knowledge of medicinal plants was held by 49.6% of farmers, 11.1% of traders, 41.7% of housewives, and 57.1% of government employees. Additionally, moderate conventional knowledge was found in 2.9% of traditional healers, 48% of farmers, 88.9% of traders, 58.3% of housewives, and 42.9% of government workers.
All traders and government employees rated medicinal plants as highly effective. Traditional healers (97.1%), farmers (96%), and housewives (83.3%) also rated these plants highly effective, whereas only 4% of farmers and 16.7% of housewives rated them as moderately effective.
Influence of income level on the frequency of use of medicinal plants
The frequency of medicinal plant use was significantly correlated with income levels. Among the respondents classified within the low-income demographic, there was unanimous (100%) reporting of regular medicinal plant usage, with 80.90% utilizing these remedies consistently, 12.60% doing so occasionally, and 6.50% infrequently. This group’s economic barriers hinder their access to modern medicine, leaving individuals to rely mainly on natural remedies, such as medicinal plants. Their reliance on environmental resources and economic difficulties leads to regular utilization of these plants for health management.
Diversity of medicinal plants used by the community
The present study, which involved rigorous face-to-face interviews and individual discussions with local herbalists and community members, provides a comprehensive record of the conventional medicinal plants used by the community. The plants have been sorted according to the alphabetical order of their families, including 105 medicinal plants belonging to 53 families (Table 3). Moreover, the Tripuri people have a unique approach to preparing conventional medicine. They collect wild and rare plant species from the reserve forest areas, which belong primarily to 11 families such as Lamiaceae, Asteraceae, Fabaceae, Acanthaceae, Apocynaceae, Malvaceae, Amaryllidaceae, Araceae, Phyllanthaceae, Rubiaceae, and Rutaceae—as revealed in the present study. Some villagers recognize the need for modernization and have initiated their cultivation in home gardens. They have also been found to transmit such knowledge of traditional phytomedicine not only to their next of kin but also to neighbours and relatives, preserving conventional medicinal practices. This long-term vision appears to set them apart from other communities in northeast India’s Tripura state, underscoring their commitment to protecting the natural treasure of medicinal plants.
Novelty of the study and cross-cultural comparison
This study analyses 105 plant species and relates them with 27 relevant published studies from various regions of India. Emphasis is placed on representative research, especially from less-represented areas or communities, to provide a better context for the uniqueness of the present findings (Table 4). This comparative analysis enables an assessment of the disparities in medicinal plant species utilized across different geographical areas in India, using the Jaccard Index (JI). The observed JI values range from 1.15 to 15.84 (Table 4). The highest JI value of 15.84 was recorded in Barpeta district, Assam, followed by Cooch Behar district, West Bengal (JI = 14.15), Dindigul, Tamil Nadu (JI = 11.93), Tirunelveli hills of Western Ghats (JI = 11.80), and Kanyakumari, Tamil Nadu (JI = 10.65). The considerable similarity noted in Barpeta, Assam, may be attributed to its geographical characteristics and the analogous vegetation in both locales, with 19 plant species identified as common to both. Cooch Behar, located in West Bengal and Tripura, shares similar climatic conditions, characterized by considerable rainfall, wet deciduous to semi-evergreen forests, and subtropical to tropical temperatures. Ethnomedicinal knowledge is primarily transmitted orally in both Cooch Behar and Tripura, maintaining customary plant usage patterns across generations and geographical areas, particularly among linguistically or culturally related populations. Additionally, the Tirunelveli hills and Kanyakumari share many similarities with the Tripuri community of Tripura regarding the use of medicinal plants, as suggested by the JI values. These similarities could be due to comparable ecological conditions, the availability of plants, common health concerns, their needs, and their distinct yet converging traditional healing practices. The minimum JI for the Gingee hills in Villupuram district, Tamil Nadu, India (JI = 1.15), was determined, revealing only three common plants due to its semi-arid to dry sub-humid climate. In contrast, Tripura has a variety of floristic compositions that contribute to the presence and use of local medicinal plant species. On the other hand, the Gingee hills are located in the Tamil Nadu region of the Eastern Ghats, known for their arid and biologically diverse forest ecosystems. Furthermore, the Malayali tribes that dominate the Gingee hills have distinct medicinal systems and practices, which foster similarity among the populations.
The present study has explored how the Tripuri community interprets the similarities and differences in the use of medicinal plants, aiming to establish cross-cultural commonalities and distinctions among the various communities concerning the utilization of medicinal plants. Compared to the Saperas/Nath community of Khetawas, the Saperas/Nath community shares eight plant species with the Tripuri community. Three species have similar uses, while five have different utilities. Plants like Aloe vera, Cuscuta reflexa, and Datura metel exhibit shared uses among both communities. In contrast, Mesua ferrea, Mimosa pudica, Peperomia pellucida, Punica granatum, and Tinospora cordifolia are utilized differently by the Saperas/Nath community [23]. Examining how Saperas/Nath and Tripuri communities interact with these shared species uncovers notable similarities and differences in their ethnobotanical views. The three plants with common uses highlight a shared understanding of specific plant qualities, underscoring a collective appreciation for their medicinal or practical benefits. Conversely, the five species with distinct applications illustrate the unique cultural and ecological influences that define each community’s relationship with nature. In contrast, the Kani tribes use Clerodendrum infortunatum to relieve itching, while Clitoria ternatea is utilized for wound healing [24]. Meanwhile, the Tripuri tribe employs Clerodendrum infortunatum to manage rheumatoid arthritis and constipation and treat type II diabetes, malaria, insect bites, and snake bites. They also use Clitoria ternatea for diabetes and jaundice, but they additionally apply it to aid in weight loss, enhance skin radiance, and improve memory retention. The Kani and Tripuri tribes utilize these plants in notably distinct ways due to their unique cultural perspectives and local health priorities. The Kani approach is a practical healing method rooted in personal medicinal knowledge, focusing on acute, visible symptoms such as itching and wound healing. In contrast, the Tripuri use these plants to address broader health issues and enhance overall well-being, targeting conditions like diabetes, memory loss, and skin radiance. This reflects a metaphorical and holistic view of health that encompasses mental, physical, and aesthetic dimensions. These variations highlight how belief systems and cultural interpretations impact indigenous knowledge of medicinal plants. The Reang community in Tripura employs four specific medicinal plants, akin to the Tripuri community: Andrographis paniculata, Ageratum conyzoides, Senna alata, and Peperomia pellucida. Additionally, both communities utilize a broader spectrum of plants, including Phlogacanthus thyrsiflorus, Homalomena aromatica, Blumea lanceolaria, Eclipta prostrata, Mikania cordata, Cuscuta reflexa, Kalanchoe pinnata, Euphorbia hirta, Mentha arvensis, Ocimum tenuiflorum, Urena lobata, Plumbago zeylanica, and Lantana camara, but have distinct utility [25]. Despite their geographical proximity within the state, the two communities employ different approaches to utilizing these medicinal plant species, reflecting their particular cultural and spiritual frameworks. The Reang community’s practices are rooted in animistic and shamanic beliefs. In contrast, Hinduism and Ayurvedic principles influence the Tripuri community’s methodologies, emphasizing healing through the attainment of internal equilibrium, overall wellness, and enhancement of health outcomes. The residents of Thoppampatti village in Tamil Nadu and the Tripuri tribe utilize twenty-one plant species: seven for the same purposes (Andrographis paniculata, Calotropis gigantea, Catharanthus roseus, Cajanus cajan, Mentha arvensis, Cyclea peltata, and Piper longum) and fourteen in diverse ways (Plumeria rubra, Momordica charantia, Ricinus communis, Clitoria ternatea, Leucas aspera, Ocimum tenuiflorum, Bombax ceiba, Hibiscus rosa-sinensis, Psidium guajava, Boerhavia diffusa, Cynodon dactylon, Cardiospermum halicacabum, Datura metel, and Lantana camara). This diversity underscores that the medicinal uses of plants are influenced by their pharmacological properties, as well as cultural, geographical, and epistemological factors. Frequently shared uses reflect the observable effects of these plants, whereas the variations point to specific health beliefs, spiritual customs, common local ailments, and the transmission of traditional knowledge within each community that shape their understanding and use of these plants. Conversely, the Banraji community of Uttarakhand exhibits similarities with the Tripuri tribe in utilizing the plants Ricinus communis and Tinospora cordifolia. However, they demonstrate unique applications for Aloe vera, Boerhavia diffusa, Calotropis gigantea, Euphorbia hirta, Mentha arvensis, Oxalis corniculata, and Terminalia chebula. The two communities differ culturally and geographically, yet they utilize Ricinus communis and Tinospora cordifolia, underscoring a common acknowledgement of these plants’ extensive therapeutic benefits for inflammation, fever, and jaundice. In contrast, the varying uses of seven species indicate different cultural interpretations shaped by local diseases and beliefs. These differences reflect how each society’s disease prevalence, cultural belief, environmental interactions, and practical applications affect their ethnobotanical knowledge. The Abotani tribe in Arunachal [26] and the Sahariya tribe in Madhya Pradesh [27] share three and two taxa, respectively, that align with those found in the Tripuri tribal medicine system. The smaller number of taxa indicates the geographical and climatic differences between the three communities, leading to distinct floral diversity and uniqueness. The Kani tribe in Kanyakumari shares thirteen plant species with the Tripuri tribe. Three species, Ricinus communis, Piper longum, and Ocimum gratissimum, are used similarly. The remaining ten species, which have distinct uses, include Cardiospermum halicacabum, Ananas comosus, Andrographis paniculata, Centella asiatica, Clitoria ternatea, Euphorbia hirta, Leucas aspera, Ocimum tenuiflorum, Tinospora cordifolia, and Vitex negundo [30]. The connections between humans and plants are widespread and deeply embedded in culture, illustrated by the ethnobotanical similarities between the Kani and Tripuri tribes. These variations highlight how each tribe’s distinct cultural perspective influences their understanding of nature, while their shared use of specific plants underscores a recognition of biological effectiveness that surpasses cultural differences. The Native communities in the Kashmir Himalayas share just two common taxa (Mentha arvensis and Cynodon dactylon). This indicates varying applications among the Tripuri community, highlighting cultural differences driven by climate and local requirements. Since Kashmir is situated at a high altitude and experiences colder temperatures than Tripura, it shows a disparity in floral growth and the utilization of specific plants for particular illnesses. The Baiga, Kharwar, and Gond tribes from the Vindhyan highlands of Uttar Pradesh share fifteen taxa with the Tripuri tribes. Among these, six species—Bombax ceiba, Catharanthus roseus, Mimosa pudica, Plumbago zeylanica, Terminalia chebula, and Zingiber officinale—are used similarly, while nine species–Andrographis paniculata, Boerhavia diffusa, Clitoria ternatea, Lantana camara, Nyctanthes arbor-tristis, Oxalis corniculata, Shorea robusta, Terminalia bellirica, and Tinospora cordifolia—serve different purposes [32]. The 15 plant species employed by the Tripuri tribes of Tripura and the Baiga, Kharwar, and Gond tribes from the Vindhyan highlands represent a well-established pan-Indian ethnobotanical knowledge system. These tribes utilize these plants in diverse ways, largely due to differences in their oral traditions, local
environmental conditions, cultural beliefs, and specific health requirements. Therefore, the varied applications of these species emerge from each tribe’s distinct interpretation and utilization of plants, which are influenced by their respective environments and healing methodologies. The Karanja community of Wardha district, Maharashtra, India, shares nine plant species in common with the Tripuri tribes, of which Aloe vera, Andrographis paniculata, Calotropis gigantea, Cuscuta reflexa, and Vitex negundo have similar uses. At the same time, the Karanja community utilizes Cynodon dactylon, Kalanchoe pinnata, Mimosa pudica, and Ricinus communis in different ways [33]. Such similar utilization reflects potential medicinal benefits, while local beliefs, needs, and cultural identity shape others. This is evident in the ethnobotanical similarities between the Tripuri and Karanja populations, showcasing the rich knowledge and diverse interpretations present in India’s traditional medicinal system. Inhabitants of Pauri district share eighteen plant taxa with the Tripuri tribe, including five species: Aloe vera, Boerhavia diffusa, Centella asiatica, Euphorbia hirta, and Mentha arvensis, which serve similar purposes. The other thirteen species—Mimosa pudica, Ocimum tenuiflorum, Plumbago zeylanica, Portulaca oleracea, Punica granatum, Swertia chirayita, Terminalia bellirica, Terminalia chebula, and Vitex negundo—have varied uses [32]. This reflects the local health priorities and demonstrates how communities uniquely utilize medicinal plants. The Gaddi tribal community in Himachal Pradesh shares three common plant taxa with the Tripuri tribe; however, their applications vary. This highlights that both communities maintain unique traditional uses for medicinal plants, influenced by their tradition, healing practices, and cultural values. The Thadou, Meitei, and Maring communities in Manipur have ten plant taxa in common with the Tripuri tribes. While one species (Centella asiatica) is used similarly by both communities, the other nine (Bischofia javanica, Euphorbia hirta, Leucas aspera, Oxalis corniculata, Paederia foetida, Phyllanthus urinaria, Portulaca oleracea, Terminalia chebula, and Vitex negundo) [36] are utilized differently due to the unique traditions and cultures of the Manipur communities, which highlight their distinct approaches to medicinal plant use. On the other hand, Inhabitants of Barpeta district, Assam, have five plant species, including Ananas comosus, Cajanus cajan, Mikania micrantha, Ricinus communis, and Tinospora cordifolia, which are utilized similarly, while Aloe vera, Centella asiatica, Eclipta prostrata, Hibiscus rosa-sinensis, Houttuynia cordata, Mimosa pudica, Ocimum gratissimum, Oxalis corniculata, Paederia foetida, Psidium guajava, and Vitex negundo have dissimilar utilization [37]. These two communities demonstrate that ethnobotanical overlap and distinct utilization of plant species reflect cultural adaptation shaped by the local inhabitants’ unique experiences, beliefs, and needs. This emphasizes the diverse expressions of traditional knowledge, even among neighbouring groups.
The tribal people of Pakyong, Sikkim, have six plant species in common with the Tripuri community. Among these, they share three similar species—Aloe vera, Bombax ceiba, and Centella asiatica—and utilize three distinct ones: Ananas comosus, Cynodon dactylon, and Cuscuta reflexa [38]. These species demonstrate a combination of common functional insights and distinct cultural adaptations shaped by geography, traditions, and ecological experiences. The Kuravas and Irulas of the Gingee hills in Tamil Nadu share three plant species with the Tripuri community. Among these, only Cardiospermum halicacabum serves similar purposes, while Clitoria ternatea and Plumbago zeylanica lack comparable uses [39]. This suggests that geographical separation plays a role, as the medicinal applications of plants are deeply rooted in the community’s cultural beliefs and the prevalent diseases specific to that area. The Kani tribes of the Tirunelveli hills in the Western Ghats share seventeen plant species with the Tripuri community, of which only three have similar uses: Cardiospermum halicacabum, Centella asiatica, and Ricinus communis. In contrast, Aloe vera, Clitoria ternatea, Cynodon dactylon, Datura metel, Euphorbia hirta, Hibiscus rosa-sinensis, Hygrophila auriculata, Leucas aspera, Mimosa pudica, Ocimum tenuiflorum, Punica granatum, Sesbania grandiflora, Terminalia chebula, and Vitex negundo do not share similar uses with the Tripuri community [40]. The prevalence of plant species can be linked to tropical and monsoon climates; however, communities in these two biodiversity hotspots face geographical differences that hinder the sharing of medicinal plants’ knowledge. As a result, each community has developed different applications for the same medicinal plants, tailored to the specific needs of its unique environment. The Mawasi tribes in the Chitrakoot district of Madhya Pradesh share six plant species, among which only Centella asiatica serves a similar purpose. In contrast, Bombax ceiba, Cynodon dactylon, Euphorbia hirta, Terminalia chebula, and Vitex negundo have distinct uses [41]. Conversely, the Irula tribes in the Nilgiri biosphere of the Western Ghats possess just two species in common: Andrographis paniculata, which serves a similar purpose, and Drynaria quercifolia, with a different function. The Chakma community in Tripura shares only two species of medicinal plants (Centella asiatica and Plumeria rubra) in common with the Tripuri community. However, there is a notable lack of similarity in the utilization of these species, indicating that community beliefs play a significant role in the application of medicinal plants for managing ailments, despite geographical proximity. This suggests that a comparative study of the traditional medicinal systems within the same geographical region may reveal divergent applications of medicinal plants for addressing similar types of ailments. The tribal inhabitants of Cooch Behar, West Bengal, share fifteen plant species that serve four similar uses and eleven distinct applications compared to the Tripuri community’s medicinal system. Species such as Cajanus cajan, Calotropis gigantea, Heliotropium indicum, and Ricinus communis exhibit similarities in utilization with the Tripuri community. At the same time, Ageratum conyzoides, Andrographis paniculata, Centella asiatica, Eclipta prostrata, Euphorbia hirta, Hibiscus rosa-sinensis, Ocimum gratissimum, Plumbago zeylanica, Psidium guajava, Sesbania grandiflora, and Vitex negundo have distinct applications [44]. The Binjhal tribes in Bargarh district, Odisha, rely on a single species (Ricinus communis) for their uses, which aligns with the practices of the Tripuri community. In contrast, they also utilize Aloe vera, Boerhavia diffusa, Bombax ceiba, Hibiscus rosa-sinensis, Terminalia bellirica, and Vitex negundo; however, the utilization of these plants differs from that of the Tripuri community, reflecting the marked indigenous healing practices of the Binjhal tribes [45]. The Mizo tribes of Champai area, Mizoram, share a significant botanical heritage with the Tripuri tribes, identified by the common presence of fifteen plant species. Of these, eleven exhibit similar applications in traditional practices, which include notable species such as Aloe vera, Cajanus cajan, Catharanthus roseus, Chromolaena odorata, Mentha arvensis, Mesua ferrea, Mikania micrantha, Mimosa pudica, Psidium guajava, Punica granatum, and Zingiber officinale. In contrast, four additional species, namely Ananas comosus, Bischofia javanica, Centella asiatica, and Houttuynia cordata, are identified, though their utilization appears to diverge from the majority [46]. This observation suggests a substantial intercultural exchange of medicinal plants, likely attributed to historical migrations and cross-border interactions between these neighbouring provinces. Such exchanges highlight the dynamic interplay of culture and botany in shaping traditional medicinal practices within the region. In contrast, the Tribes of Keonjhar in Orissa have only two species in common, Terminalia chebula and Shorea robusta, each fulfilling a unique role [47]. Meanwhile, the Monpa tribes of Arunachal Pradesh share eight species, categorized into four with similar uses (Momordica charantia, Psidium guajava, Punica granatum, and Zingiber officinale) and four others (Ageratum conyzoides, Centella asiatica, Houttuynia cordata, and Leucas aspera) with different applications [48]. Lastly, the tribes of Datia in Madhya Pradesh have seven common species, consisting of four (Ageratum conyzoides, Centella asiatica, Lantana camara, and Psidium guajava) with similar uses, and three (Clitoria ternatea, Oxalis corniculata, and Tinospora cordifolia) with differing applications [49].
Following a comparison of the findings of the current study with 27 selected published reports, it has been observed that 42 plants have rarely been documented for treating human ailments within the examined ethnobotanical literature: Jusitical gendarussa, Alternanthera brasiliana, Allium tuberosum, Crinum asiaticum, Hymenocallis littoralis, Cosmonstigma cordatum, Alocasia indica, Typhonium trilobatum, Licuala spinosa, Dracaena trifasciata, Drimia indica, Diplazium esculentum, Acmella uliginosa, Gnaphalium pensylvanicum, Impatiens balsamina, Distimake vitifolius, Chamaecostus cuspidatus, Hellenia speciosa, Bauhinia acuminata, Senna siamea, Anisochilus carnosus, Callicarpa longifolia, Clerodendrum chinense, Leucas lavandulifolia, Premna bengalensis, Yamazakia viscosa, Abroma augustum, Melastoma malabathricum, Jasminum officinale, Averrhoa carambola, Breynia androgyna, Thyrsostachys oliveri, Persicaria viscosa, Pontederia vaginalis, Mitragyna speciose, Discospermum sphaerocarpum, Citrus assamensis, Clausena excavate, Murraya intermedia, Talinum fruticosum, and Debregeasia longifolia. The presence of underreported medicinal plant species implies the potential to discover new phytocompounds and represents a unique traditional pharmacopeia. Validating such plants may pave the way for the development of new therapeutic agents.
Cross-geographical analysis
In the fringe villages of UURF, Chromolaena odorata, Leucas lavandulifolia, Breynia androgyna, and Portulaca oleracea hold significant indicator value (Fig. 2). This is mainly because these plants are commonly found in the nearby villages and serve multiple purposes. While Alternanthera brasiliana, Centella asiatica, Catharanthus roseus, Licuala spinosa, Dracaena trifasciata, Cuscuta reflexa, Momordica charantia, Euphorbia hirta, Senna alata, Senna siamea, Yamazakia viscosa, Bombax ceiba, Boerhavia diffusa, Peperomia pellucida, Paederia foetida and Debregeasia longifolia (Fig. 2) are the indicator species of DRF. All these plant species have a significant utilization (p < 0.05) in the fringe villages of DRF, as they are commonly observed there. They also have good medicinal value, particularly against gastrointestinal ailments, cold, cough, and joint pain-related issues. However, the neighbouring villages of DURF lack any indicator species. This absence may result from their geographical location between the other two reserve forests and their relatively small size. Five adjacent villages have a notable number of Tripuri community members, although this population is smaller than the fringe villages of the other two neighbouring reserve forests. The variation in indicator species between the UURF and the DRF may be linked to differing edaphic factors such as soil moisture, pH, moisture retention capacity, and nutrient content, along with the essential microclimatic conditions that support the growth of medicinal plants. Nonetheless, additional research is necessary to clarify the underlying reasons for these differences and form a comprehensive epilogue.

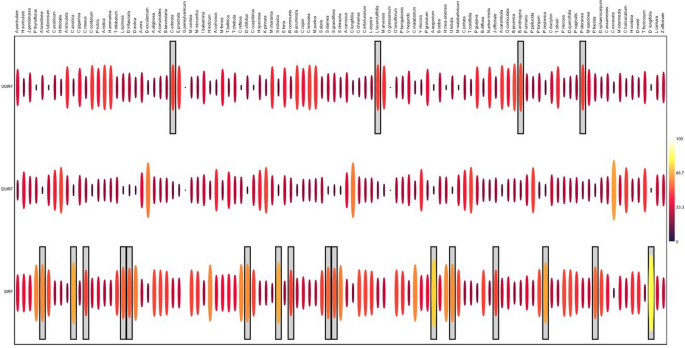
Values of indicator species across three reserve forest clusters are emphasized in the box, covering three distinct survey areas
Family-wise diversity of medicinal plants and the process of their application
The study area under consideration featured an intriguing distribution of plant families (Fig. 3), with Lamiaceae emerging as the most prolific family, showcasing 11 observed species. Asteraceae followed closely, with 8 species. The Fabaceae family ranked third, with 7 species observed. Acanthaceae, Apocynaceae, and Malvaceae families each recorded 4 species. Amaryllidaceae, Araceae, Phyllanthaceae, Rubiaceae, and Rutaceae families were represented by 3 species each. Other families, including Asparagaceae, Combretaceae, Convolvulaceae, Costaceae, Euphorbiaceae, Menispermaceae, Oleaceae, Oxalidaceae, Piperaceae, and Poaceae, represented 2 species each. In contrast, the remaining families exhibited only 1 species in the study area (Fig. 3, Supplementary File 1). This study area is a valuable repository of diverse plant families and species. Therefore, it is essential to conserve such an ecosystem so that future generations can benefit from and experientially learn about its ecological significance. Leaves constituted the most collected specimens and the utilized plant part, accounting for 38% of the total. This is because they are the easiest to obtain and the most readily accessible portion of the plant. Leaves also contain the highest phytochemical components for treating various ailments [21]. Flowers were the second most collected plant parts, accounting for 15%, followed by fruits (11%), whole plants and stems (8%), roots (6%), rhizomes (5%), seeds (4%), barks (3%), shoots (2%), bulbs (1%), pulp (0.5%), pods (1%), twigs (0.1%), latex and inflorescence (0.1%), respectively. In the study, herbal treatments have been noted to be prepared using 13 distinct processes. Poultice and infusion were the most popular methods, accounting for 24% and 23% of usage, respectively. The third most used method was sap (19%), followed by decoction (16%), crude extract (5%), cooked as a vegetable (4.5%), juice (2.6%), oil (2.3%), tea (1.3%), ripened fruit, and chewing of bark or stem either in dried or raw form (0.7%), raw leaves (0.5%), and powder (0.4%).


Family-wise dominance of medicinal plants used by the Tripuri community in Unakoti district, Tripura, northeast India
The chord diagram (Fig. 4) effectively showcases the complex connections between different plant parts used in traditional medicine and their application methods. Leaves are the most frequently used, commonly linked with preparations like infusion, decoction, and poultice, highlighting their central role in ethnomedicinal practices. Flowers, fruits, and roots also have significant associations, especially with sap and juice usage. The diagram emphasizes that infusion and poultice remain the primary methods, reflecting their popularity in extracting or applying bioactive compounds. Less frequently used parts, such as twigs, latex, and inflorescence, have limited representation, indicating specialized roles. This visual tool not only displays usage frequency but also reveals preferred combinations, offering valuable insights into traditional pharmacological knowledge and helping identify key bioresource components for future phytochemical and pharmacological studies.


The diagram shows the relationships between various plant parts used by the Tripuri tribes and how they are applied. Connecting chords indicate the frequency and strength of the association between specific plant parts and application processes. Thicker chords represent more frequently reported combinations
Agreement on medicinal plants for common diseases in the study area
ICF serves as a metric for evaluating the efficacy of plant species in treating specific ailments. Higher ICF values denote a widespread consensus among informants regarding the effectiveness of a particular plant in addressing an illness. Conversely, lower ICF values indicate a lack of unanimity among informants concerning the suitability of plants for addressing specific diseases [50]. This study calculates the ICF values to evaluate the significant plants the Tripuri community uses to manage various diseases. The community employs a diverse range of traditional techniques to treat various ailments. As shown in Table 5, eighty-three (83) illnesses were segmented into 14 use categories, wherein pregnancy and childbearing were found to have the highest ICF value of 1.0, followed by respiratory, digestive, musculoskeletal, neurological, blood, skin, psychological, endocrine, urinary, general, eye, circulatory, and genital systems, with ICF values ranging from 0.97 to 0.98. Medics and researchers continually pursue more effective treatment strategies for various illnesses. The present study has uncovered valuable information to aid them in this endeavour. The informants agreed upon the medicinal plants and their uses against specific ailments, indicating high confidence in their effectiveness.
link